

Accuracy Requirements of 3D Printed Models in Dentistry
This document aims to establish a comprehensive understanding of the dimensional accuracy requirements of models used in dentistry. Additive manufacturing has evolved from a rare alternative into a standard practice within the dental industry. However, this transition has not been fully mirrored in the industry’s standardization and norms. As a leading hardware and materials manufacturer, Formlabs Dental is committed to staying ahead of the competition by understanding both the explicit and implicit norms that guide the specialized dentistry sector. Traditional norms and expectations, while foundational, often lag behind the rapid advancements in digital workflows and Computer-Aided Manufacturing (CAM) technologies. The objective of this paper is to assess what researchers have determined to be clinically acceptable, and what constitutes an adapted gold standard in the context of our current 3D printing technology’s capabilities and limitations.
Accuracy Requirements of 3D Printed Models in Dentistry
This document aims to establish a comprehensive understanding of the dimensional accuracy requirements of models used in dentistry. Additive manufacturing has evolved from a rare alternative into a standard practice within the dental industry. However, this transition has not been fully mirrored in the industry’s standardization and norms. As a leading hardware and materials manufacturer, Formlabs Dental is committed to staying ahead of the competition by understanding both the explicit and implicit norms that guide the specialized dentistry sector. Traditional norms and expectations, while foundational, often lag behind the rapid advancements in digital workflows and Computer-Aided Manufacturing (CAM) technologies. The objective of this paper is to assess what researchers have determined to be clinically acceptable, and what constitutes an adapted gold standard in the context of our current 3D printing technology’s capabilities and limitations.
The Gold Standard of Prosthetic Dental Plaster Models
When engaging with dental professionals, two key insights emerge: first, there is no universally established standard defining clinically acceptable accuracy for models; second, traditional stone plaster models are widely regarded as the gold standard.
In 1984, the International Organization for Standardization (ISO) stepped in to bring some much-needed consistency to the dental industry, specifically regarding dental plaster. Before this, there was a lot of variation in what was considered the right level of accuracy for a dental model, influenced by factors like regional practices, individual training, and hands-on experience. The ISO addressed this by introducing the ISO 6873 [11] standard. The last revision, released in 2013, lays out clear requirements and methods for testing dental plasters. However, before delving into these specifics, it is essential to first examine the accuracy of patient dentition and oral anatomy impressions, as these form the foundational data input for model production.
How Accurate Can a Traditional Impression Be?
The accuracy depends on several factors such as:
- Type of tray (custom or stock)
- Impression material (PVS, polyether, alginate)
- Experience of the person taking the impression
- Patient anatomy
- Patient movement / lack of cooperation
- Humidity control during impression taking
- Single-phase and two-phase impression techniques
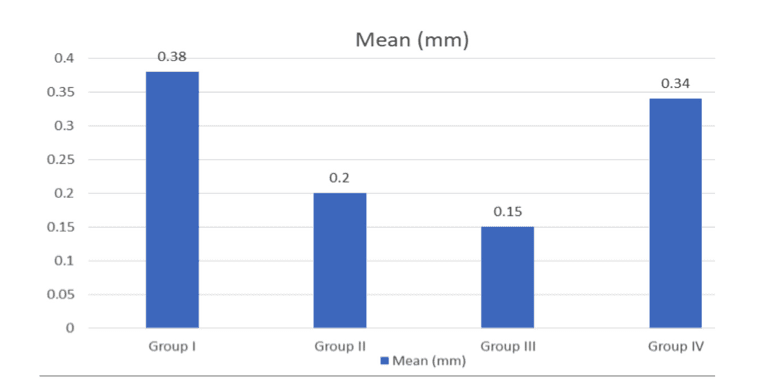
Impression quality can vary a lot. “Accuracy of different materials used in impressions for fixed partial dentures” by Dr. Farhat Jabeen, Dr. Pratibha Sharma, and Dr. Paritosh Sharma [8] indicates that the accuracy of traditional impressions will offer a mean trueness of 0.25 mm (averaging different impression materials where polyether is the most precise and condensation silicone the least). Hence, comparing the accuracy of dental models produced with traditional techniques and with additive manufacturing needs to take into account the workflow and success rate of each method.
How Accurate Can an Intraoral Scan Be?
The Type IV ISO 6873 for stone plaster models is based on traditional impressions. Based on studies such as the one by Dr. Farhat Jabeen et al. [8], we can calculate a cumulative mean absolute deviation for the accuracy of the model produced with this workflow. When we shift focus to 3D printed models, the workflow diverges significantly. Although there are hybrid methods that blend traditional impression-taking with digital model creation, a direct comparison between traditional and fully digital workflows necessitates an examination of the accuracy of the initial data acquired. In a fully digital context, this data originates from an intraoral scanner.
Research articles by Kernen, Schlager et al. [9] and Winkler et al. [10], shed light on varying accuracy levels in this domain. The study by Kernen, Schlager et al. [9] evaluates the trueness and precision of full-arch in vivo scans using different scanner models. A notable discrepancy emerges when comparing the accuracy of full-arch scans to smaller sections, underscoring a recognized challenge in intraoral scanning. The limited field of view of intraoral scanners requires stitching algorithms to compile multiple smaller views into a comprehensive model. This often results in diminished accuracy over larger spans.
The study by Winkler and Gkantidis [10] presents a contrasting perspective, showcasing remarkable accuracy in scanning smaller sections (such as the front teeth of the upper arch) compared to a full-arch scan. However, this fidelity diminishes when assessing full-arch accuracy. For instance, the trueness of TRIOS 3 scans, with a 0.065 mm Mean Absolute Deviation (MAD), lags behind the performance of polyvinyl siloxane (PVS) impressions noted in study [8], which achieved a 0.02 mm MAD.
Though these findings date back to 2020, and there have been ongoing improvements in intraoral camera technology and algorithms, this data remains pivotal in contrasting the digital dental workflow with its traditional counterpart.
Get in Touch
Whether you need to produce occlusal splints in-house, or are looking for high-throughput production of dental models, we're here to help. Get in touch with a dental expert to find the right solution for your business.
A Closer Look at ISO 6873 [11]
ISO 6873 defines high accuracy, especially for Type III and Type IV stone plaster models. Dental models come in various types, each tailored to specific requirements with varying accuracy needs depending on their intended use. Here’s an incomplete list organized from least accuracy required to highest accuracy required:
- Study models
- Documentation models
- Models for quick repairs
- Models for manual waxups
- Models for thermoforming appliances
- Models for prosthetic work
- Models for single-unit implant work
- Models for multi-unit implant work
ISO 6873:2013
| Type | Setting Expansion (%) | Compressive Strength (psi) |
| 1 |
0-0.15 |
580-1160 |
| 2 |
0-0.30 |
≥1300 |
| 3 |
0-0.20 |
≥2900 |
| 4 |
0-0.15 |
≥5100 |
In the realm of prosthetic dental work, Type III and Type IV plasters are the most commonly used materials. Type III plaster is primarily used for acrylic applications, such as dentures, while Type IV is considered the gold standard for restorative models and master casts for implants. We are going to focus on prosthetic models, so Type IV is the most relevant specification.
Two key aspects of these plasters are noteworthy in the context of the ISO 6873 standard:
-
Setting Expansion Value: One of the critical factors defined in the standard is the setting expansion. During the plaster setting process, a dimensional expansion occurs, which is why the norm focuses solely on expansion values. Contraction, or shrinkage, is generally not a concern with dental plaster, and thus, contraction values aren’t specified in the norm.
-
Measurement of Acceptable Range: The standard defines the acceptable range of expansion in percentage terms, measured linearly. This means the permissible expansion is proportional to the object’s size, making it a relative measure.
These specifications, however, present a challenge when applied to 3D printed resin models. Contrary to dental plaster, which exhibits uniform expansion, the 3D printing process can lead to both positive and negative deviations in accuracy. As a result, when assessing a 3D printed model, one must account for potential deviations that may occur in either direction. This contrasts with dental plaster, where negative deviations (contraction) are typically non-existent. This difference underscores the difficulty in directly translating these standards to 3D printed models, which require a more multidimensional approach to quality control.
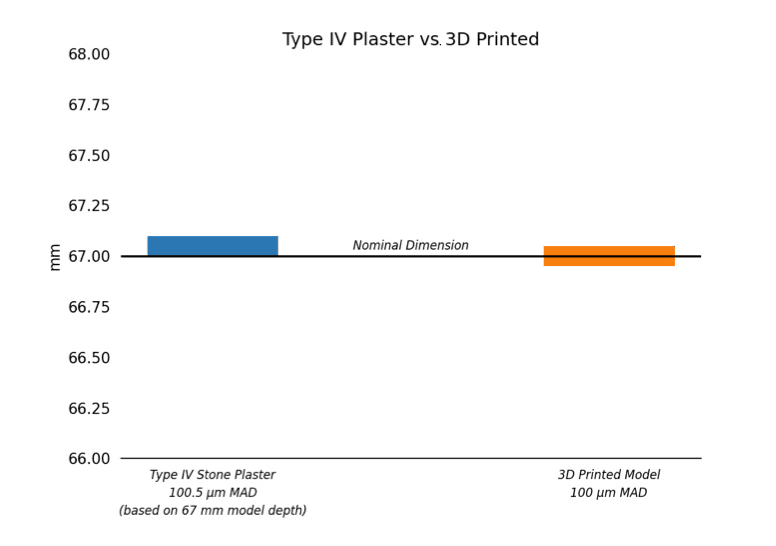
When evaluating the precision of a plaster model conforming to the Type IV standard against the accuracy of a 3D printed model, it’s important to focus on which model more consistently aligns with the nominal dimension. In this regard, the Mean Absolute Deviation (MAD) is a valuable metric as it measures the magnitude of deviation irrespective of its direction. A lower MAD in one model compared to the other indicates a closer adherence to the intended dimension, thus marking it as more accurate.
A Specific Example for a Type IV Stone Plaster Model
Let’s take, for instance, a dental arch with a sagittal depth of 67 mm, derived from the average length of several dental arches. For a plaster model meeting the Type IV criteria, the maximum permissible deviation (which, in this case, is exclusively positive) would be calculated as follows:
- Model Size: 67 mm
- Acceptable Linear Expansion: 0.15%
- Tolerance Range: 67 mm × 0.15% / 100 = 0.1005 mm
For the plaster model, the MAD is computed thus:
- Minimum Deviation (at 67 mm): |67 - 67| = 0 mm
- Maximum Deviation (at 67.1 mm): |67.1 - 67| = 0.1 mm
- MAD = (0 + 0.1) / 2 = 0.05 mm
Assessing the Accuracy of a 3D Printed Resin Model
Assuming a 3D printed model exhibits a similar range of deviation but in both directions, we would expect a similar MAD if the model is equally accurate. For a deviation range of ±0.05 mm (67 mm ±0.05 mm):
-
Minimum Deviation (at 66.95 mm): |66.95 - 67| = 0.05 mm
-
Maximum Deviation (at 67.05 mm): |67.05 - 67| = 0.05 mm
-
MAD = (0.05 + 0.05) / 2 = 0.05 mm
When considering the accuracy of 3D printed models, it’s interesting to note how this is framed at Formlabs. Accuracy is typically described in terms of “X% of the model’s surface being within a range of ±Y mm of the nominal object.” Applying this to the previous example, it would mean that “100% of the surface of the printed model falls within ±0.05 mm (50 µm) of the nominal dimension.” This approach, while simplified, offers a practical and informative way to gauge and contrast the precision of various manufacturing techniques used in creating dental models.
However, translating a norm based on maximum linear expansion, such as the one used for plaster models, to the realm of 3D printing, isn’t straightforward. It involves establishing a comparative metric that takes into account the inherent limitations and characteristics of 3D printing technology. This comparison seeks to bridge the gap between different manufacturing processes, providing a common ground to evaluate their accuracy, while acknowledging that each method has its unique attributes and constraints.
What Is Clinically Acceptable?
The notion of what is clinically acceptable varies widely, and there is no universally agreed-upon standard. A systematic review by Etemad-Shahidi et al. [12] suggests that clinical acceptability ranges from under 0.1 mm to under 0.5 mm. To achieve the highest accuracy standard of less than 100 µm, both plaster models and digital workflows face challenges. In the digital workflow, the limitations of intraoral scanners and model accuracy are significant factors. A model material that prints with 100% of its surface within ±0.05 mm would mark a significant advancement. However, this only meets the benchmarks set by a few specific studies [12].
It’s crucial to recognize that a model resin achieving 100% accuracy within ±100 µm would still be less accurate than the traditional plaster standard with Type IV ISO 6873 compliance. Achieving a precision of ±50 µm would bring 3D printed dental models using Formlabs technology on par with traditional plaster models, according to these standards.
Creating a clinically acceptable dental model involves a comprehensive process that encompasses three key aspects:
-
The accuracy of the initial data or input
-
The precision of the manufacturing method
-
The trueness of the final model in relation to the input data.
It’s important to recognize that each of these stages has its inherent margin of error, cumulatively contributing to the overall accuracy of the final model. The articles reviewed and cited in this paper focus on the accuracy of various traditional impression materials and the precision of different additive manufacturing methods in the context of dental models [see appendix].

Request a Free Sample Part
See and feel Formlabs quality firsthand. We’ll ship a free 3D printed sample part printed on the Form 4B to your office.
Assessing Overall Accuracy in Dental Models
The formula for determining the absolute accuracy of the final dental model can be summarized as follows:
For instance, consider a Type IV plaster model based on a PVS impression using a custom tray and plaster mixed in a vacuum mixer according to the manufacturer’s instructions. This scenario might yield:
0.2 mm impression error + 0 mm precision error of vacuum mixed plaster + 0.05 mm accuracy error of type IV plaster = Absolute accuracy of 0.25 mm
-
Impression error of 0.2 mm (MAD) + # [7]
-
For a model of length 67 mm, a maximum error of 0.05 mm (MAD) is required by the ISO
-
We assume 0 precision error for plaster mixing using a vacuum mixer
Here, the significant contributor to error is the impression-taking process, which outweighs the accuracy of the model material itself.
In the context of 3D printing, comparable data on the accuracy of modern intraoral scanners can be found in different research articles [9], [10]. In addition to scan imperfections, the variability between prints comes into this equation.
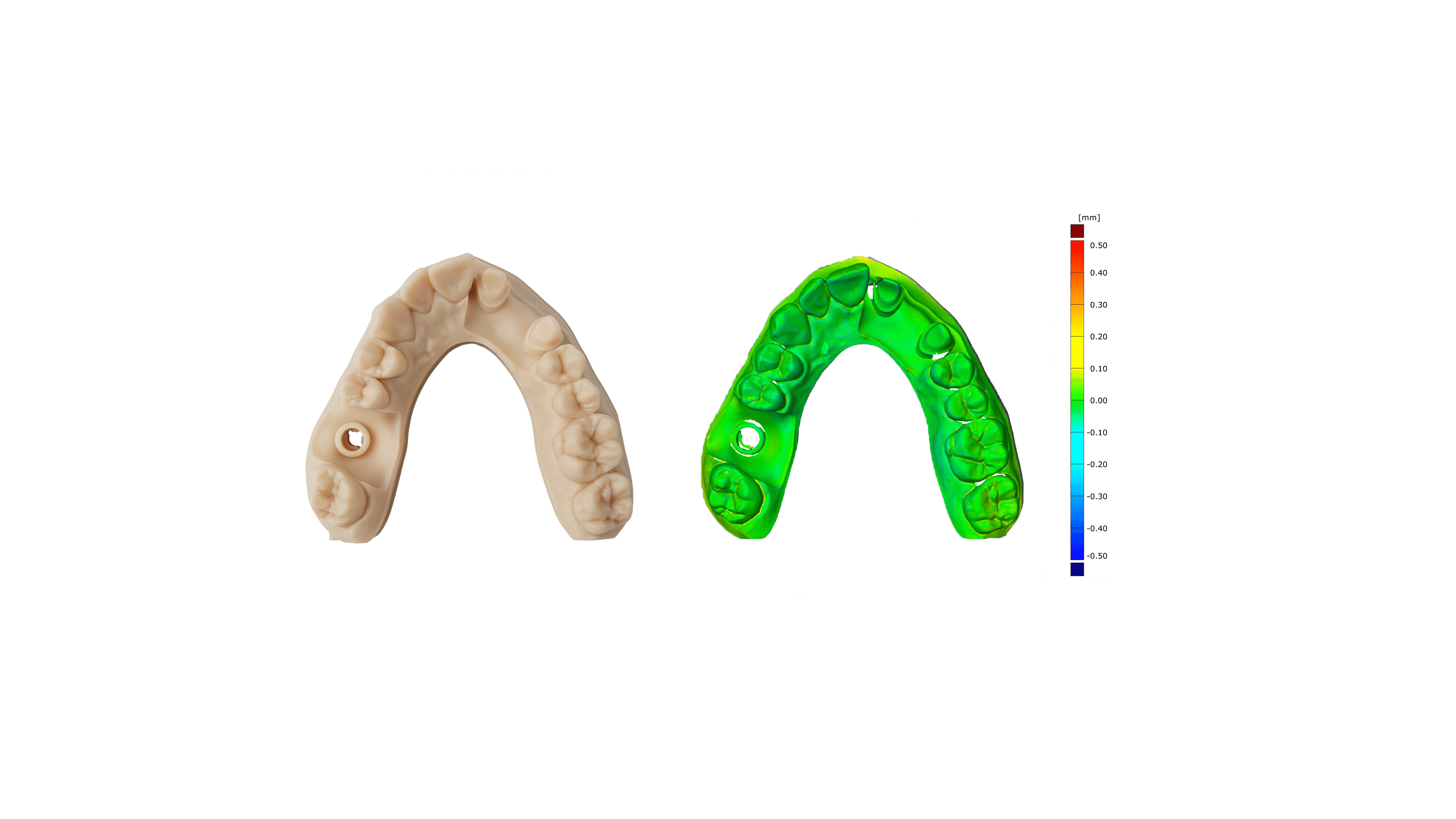
Formlabs’ Form 4B 3D printer delivers repeatable results and unmatched accuracy. Again, the calculation is for a full arch model with a depth of 67 mm printed with Precision Model Resin with a layer height of 50 µm.
Thus, the error calculation for a model printed on Form 4B might be:
0.147 mm scan error + 0 mm precision error + 0.1 mm accuracy error = Absolute accuracy of 0.25 mm
-
Scanner error is taken from Kernen, Schlager et al. [9] (3Shape TRIOS)
-
Similar to the plaster equation, we assume zero precision error from the Form 4B
-
Model accuracy of about 0.1 mm (≥95% at 50 µm layer height with Precision Model Resin)
Conclusion
In summary, precision requirements for 3D printed dental models is a landscape where traditional practices and modern technologies intersect, often with complex outcomes. Despite the widespread adoption of 3D printing in dentistry, a universal benchmark for what constitutes clinically acceptable accuracy remains elusive. Traditional stone plaster models conforming to ISO 6873 standards have long been the benchmark, yet their direct comparison with 3D printed models is not straightforward and has not yet been established.
The accuracy of traditional impressions is influenced by multiple factors, including the choice of materials and techniques, the experience of the practitioner, and patient-specific variables. 3D printed models introduce a different set of challenges, primarily due to potential deviations in dimensions during the printing process. The use of the Mean Absolute Deviation (MAD) is an attempt to gauge precision, highlighting the nuances of each method.
A key takeaway from this analysis is the recognition of the performance of Form 4B in conjunction with Precision Model Resin. While advancements are ongoing, achieving the high accuracy standards set by traditional methods is an ongoing challenge for 3D printing. With the Form 4B and Precision Model Resin, Formlabs Dental 3D printers match the industry standards set for traditional methods.
This document underscores the importance of a multi-faceted approach to accuracy in dental models. This approach considers not just the final output, but also the accuracy of initial data and the precision of the manufacturing process. As we push the boundaries of what is possible, it’s crucial to keep in mind that the ultimate goal remains the same: to ensure that dental models, whether traditionally made or 3D printed, meet the high standards required for clinical use.
Get in Touch
Whether you need to produce occlusal splints in-house, or are looking for high-throughput production of dental models, we're here to help. Get in touch with a dental expert to find the right solution for your business.

Product Demo: Form 4B
Blazing speed meets unmatched accuracy in the next generation of dental 3D printing. Explore the latest innovations in our on-demand webinar.

Request a Free Sample Part
See and feel Formlabs quality firsthand. We’ll ship a free 3D printed sample part printed on the Form 4B to your office.
Appendix
-
Papaspyridakos, P., Chen, Y. W., Alshawaf, B., Kang, K., Finkelman, M., Chronopoulos, V., & Weber, H. P. (2020). Digital workflow: In vitro accuracy of 3D printed casts generated from complete-arch digital implant scans. The Journal of prosthetic dentistry, 124(5), 589–593. https://doi.org/10.1016/j.prosdent.2019.10.029
-
Ender, A., & Mehl, A. (2013). Accuracy of complete-arch dental impressions: a new method of measuring trueness and precision. The Journal of prosthetic dentistry, 109(2), 121–128. https://doi.org/10.1016/S0022-3913(13)60028-1
-
Abdeen, L., Chen, Y. W., Kostagianni, A., Finkelman, M., Papathanasiou, A., Chochlidakis, K., & Papaspyridakos, P. (2022). Prosthesis accuracy of fit on 3D-printed casts versus stone casts: A comparative study in the anterior maxilla. Journal of esthetic and restorative dentistry : official publication of the American Academy of Esthetic Dentistry ... [et al.], 34(8), 1238–1246. https://doi.org/10.1111/jerd.12954
-
Rebong, R. E., Stewart, K. T., Utreja, A., & Ghoneima, A. A. (2018). Accuracy of three- dimensional dental resin models created by fused deposition modeling, stereolithography, and Polyjet prototype technologies: A comparative study. The Angle orthodontist, 88(3), 363–369. https://doi.org/10.2319/071117-460.1
-
Camardella, L. T., Vilella, O. V., van Hezel, M. M., & Breuning, K. H. (2017). Accuracy of stereolithographically printed digital models compared to plaster models. Genauigkeit von stereolitographisch gedruckten digitalen Modellen im Vergleich zu Gipsmodellen. Journal of orofacial orthopedics = Fortschritte der Kieferorthopadie : Organ/official journal Deutsche Gesellschaft fur Kieferorthopadie, 78(5), 394–402. https://doi.org/10.1007/s00056-017-0093-1
-
Baldissara, P., Koci, B., Messias, A. M., Meneghello, R., Ghelli, F., Gatto, M. R., & Ciocca, L. (2021). Assessment of impression material accuracy in complete-arch restorations on four implants. The Journal of prosthetic dentistry, 126(6), 763–771. https://doi.org/10.1016/j.prosdent.2020.10.017
-
Dr. Farhat Jabeen, Dr. Pratibha Sharma, Dr. Paritosh Sharma. Accuracy of different materials used in impressions for fixed partial dentures. Int J Appl Dent Sci 2022;8(1):113-115. https://doi.org/10.22271/oral.2022.v8.i1b.1581
-
Kernen, F., Schlager, S., Seidel Alvarez, V., Mehrhof, J., Vach, K., Kohal, R., Nelson, K., & Flügge, T. (2022). Accuracy of intraoral scans: An in vivo study of different scanning devices. The Journal of prosthetic dentistry, 128(6), 1303–1309. https://doi.org/10.1016/j.prosdent.2021.03.007
-
Winkler, J., & Gkantidis, N. (2020). Trueness and precision of intraoral scanners in the maxillary dental arch: an in vivo analysis. Scientific reports, 10(1), 1172. https://doi.org/10.1038/s41598-020-58075-7
-
ISO 6873:1984, ISO 6873:2013
-
Etemad-Shahidi, Y., Qallandar, O. B., Evenden, J., Alifui-Segbaya, F., & Ahmed, K. E. (2020). Accuracy of 3-Dimensionally Printed Full-Arch Dental Models: A Systematic Review. Journal of clinical medicine, 9(10), 3357. https://doi.org/10.3390/jcm9103357