
In-House 3D Printing of Occlusal Splint for Patient with Parafunctional Habits and Premature Tooth Wear
Under a traditional workflow, occlusal splint fabrication is generally delegated to the dental laboratory. There, lab technicians either mill the splints from a solid puck, or block, of material or produce them additively with 3D printing. Milled splints provide a durable, optically clear appliance, but both the material and milling equipment are more expensive than 3D printing workflows.
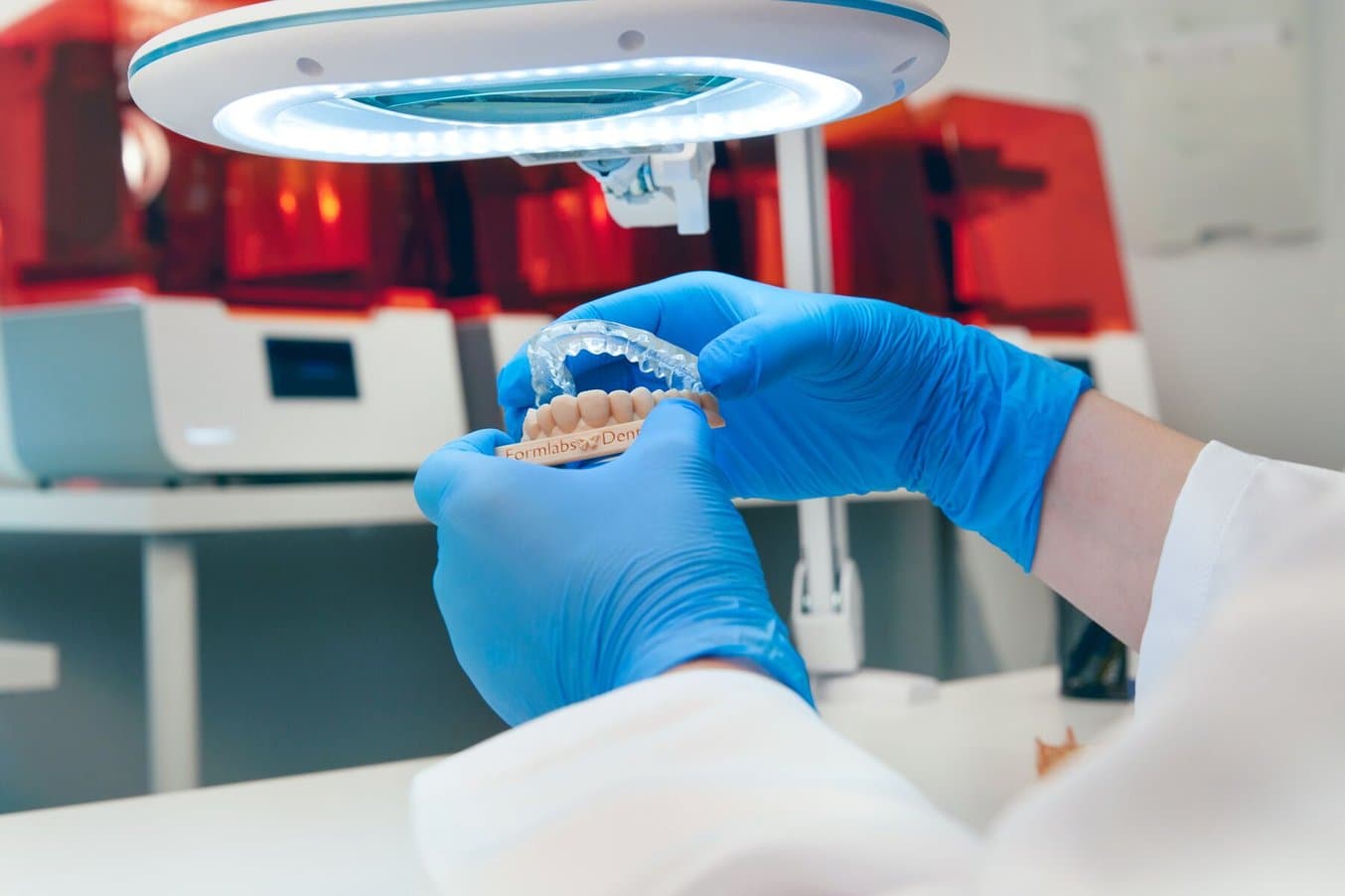
Advances in 3D scanning and 3D printing technology have enabled both labs and clinics to reduce costs and improve efficiency, without compromising on quality. 3D printing splints in-house is now possible with Dental LT Clear Resin (from Formlabs Dental) and an SLA 3D printer, such as the Form 3B+ from Formlabs Dental. Deploying 3D printing in the dental clinic not only improves turnaround time of the appliance, but allows for reductions in cost for the appliance, reduced chair time for delivery, and quick fabrication of a secondary appliance in cases of loss — i.e., “my pet ate my nightguard” — without significant additional cost. The ability to efficiently and reliably 3D print splints helps providers offer quick relief to patients suffering pain from occlusal problems.
Dr. Christopher Baer
Dr. Christopher Baer is a master at implementing digital dentistry workflows in the dental practice. He runs a fully digital dental practice in Colorado and also serves as a Formlabs Key Opinion Leader, lecturer, and advisor on digital dental technologies and implementation strategies. He has over a decade of experience developing digital dental workflows and utilizing dental technology to improve clinical efficiency.
Case Presentation and Diagnosis
A 17 year old male patient, along with his parents, presented to the dental clinic after his pediatric dentist noted that his teeth were shorter than normal. Review of medical history showed no current medications and only seasonal allergies. Dental history included orthodontic treatment that was completed at age 15 and annual dental cleanings. His last dental examination was approximately 12 months prior.
During the clinical examination, it was detected that oral hygiene was poor and patient motivation for brushing and flossing was low. Caries was noted on #9 and #10 interproximally (#21 and #22 in FDI notation/ISO 3950 notation). Evaluation of the dentition showed a parafunctional wear pattern — moderate anterior wear on the maxilla and mild wear on the mandible. The upper anterior teeth were estimated to have lost approximately 1.5 - 2.0 mm of tooth structure and the posterior bicuspids and lower anterior teeth to have lost approximately 1.0 mm. Patient reports that he sometimes wears his traditional Hawley style retainers but does not recall the last time they were worn. Patient does not report any current jaw discomfort, awareness of tooth grinding, or a visual change in the length of his teeth. Examination of the muscles of mastication and maximum jaw opening are all within normal limits and there were no joint sound or deviations of the mandible upon opening. The patient did not report any sleep sounds or disturbances with sleep, and his airway evaluation was within normal limits. When the patient and parents were informed of the parafunctional wear, they were alarmed as they stated this finding has never been mentioned by any other doctors.
Upon further questions it was determined the patient did not have any digital records from the orthodontist which, in this case, could have been valuable in assessing the final orthodontic tooth position and amounts of wear that could have occurred post orthodontic treatment, since the case was completed a few years ago. It was decided that an in-house splint would be fabricated to minimize the wear on the teeth and track the wear on the splint which can help show the parents and patient how active the parafunctional process is and if any other treatment could be necessary.

Fig 1. Intraoral picture showcasing the extensive wear.

Fig 2. Intraoral picture of the upper arch

Fig 3. Intraoral picture of the lower arch
Request a Free Splint Sample Part
Curious to see the quality firsthand? Pick a material and we'll ship you a free sample part 3D printed on the Form 3B+ to evaluate.
Treatment Plan
- Dental Prophylaxis and oral hygiene instruction
-
Caries management: Direct Dental Composite restorations on #9 and #10 (#21 and #22 in FDI notation/ISO 3950 notation)
-
Digitalization of the case via intraoral scanning (Medit i700 Intraoral) to obtain virtual 3D models for wear tracking, occlusal splint fabrication and to facilitate discussion with the parents regarding advanced wear in the 17 year-old patient.
-
Occlusal splint fabrication
Execution of Treatment Plan
First appointment: Limited to dental prophylaxis and oral hygiene instruction. Though hygiene and scanning can occur at the first appointment, it was decided to have prophylaxis and oral hygiene instruction at the first visit instead, and then have the patient return in one week to evaluate changes.
Second appointment (one week after): Dedicated to caries removal and composite restorations on #9 and #10 (#21 and #22 in FDI notation/ISO 3950 notation). Intraoral scanning was done after the composite restorations were completed to obtain virtual 3D models for occlusal evaluation in addition to occlusal splint fabrication. The occlusal records were taken in the maximum intercuspal position. The case was sent to an external design service (Evident) following the digital impressioning process with an intraoral scanner (Medit i700). The design service requires upper and lower full arch scans in addition to at least one bite scan. Upon completion of the design, the design center provides the design file and, if desired, a .Form file to simplify the print process using the native Formlabs PreForm printing software.
In-between appointments (design and fabrication stage):
-
3D printing stage: The following morning the Occlusal Splint design (.stl file) was loaded into the PreForm software and oriented for printing to the Form 3B+ printer utilizing Dental LT Clear Resin (V2). This biocompatible material is indicated for high-quality, long-term occlusal splint fabrication and a Class I (US) and Class IIa (EU) medical device.
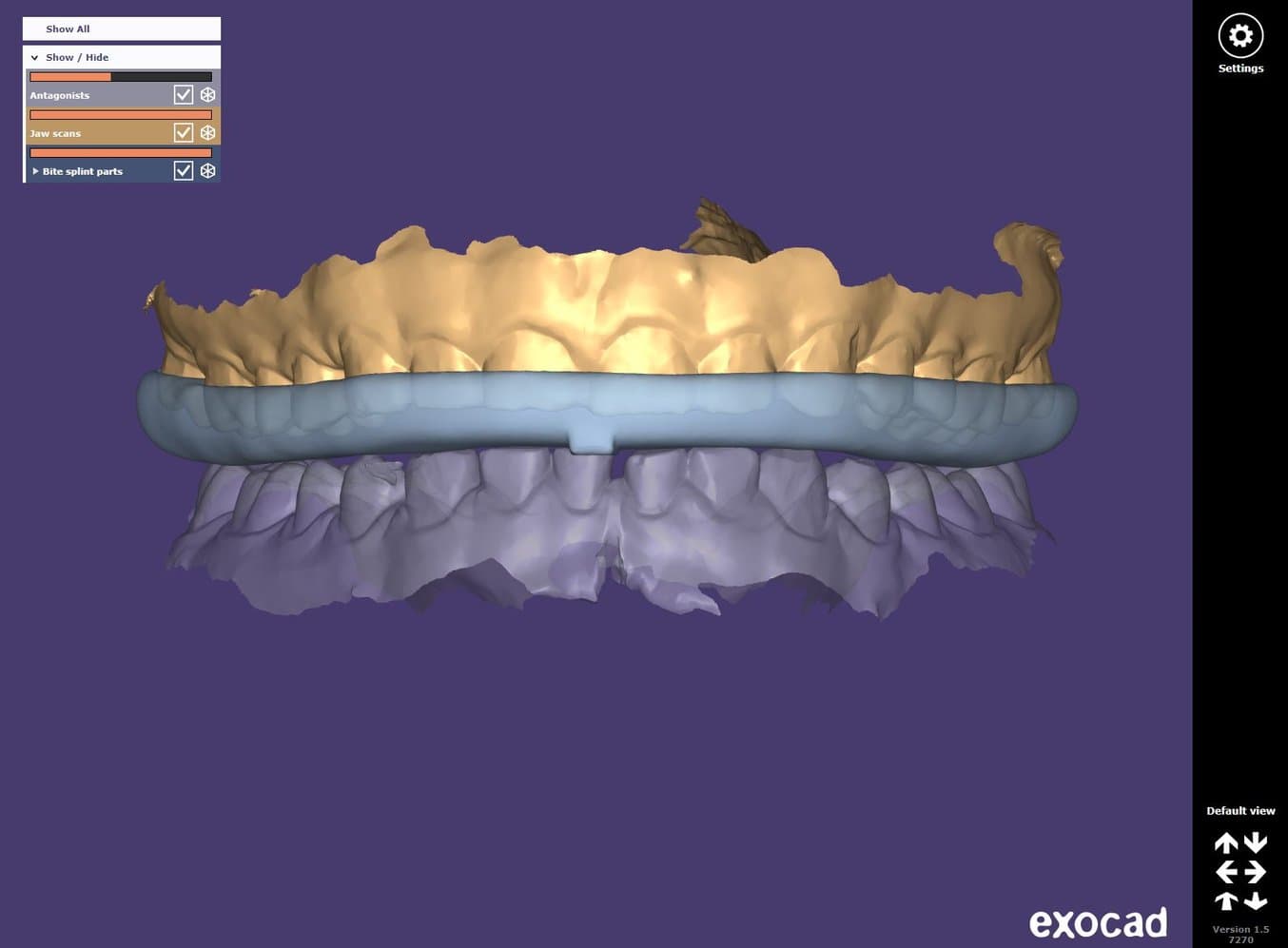
Fig 4 & 5: Occlusal splint designed in exocad by the Design Service (Evident)
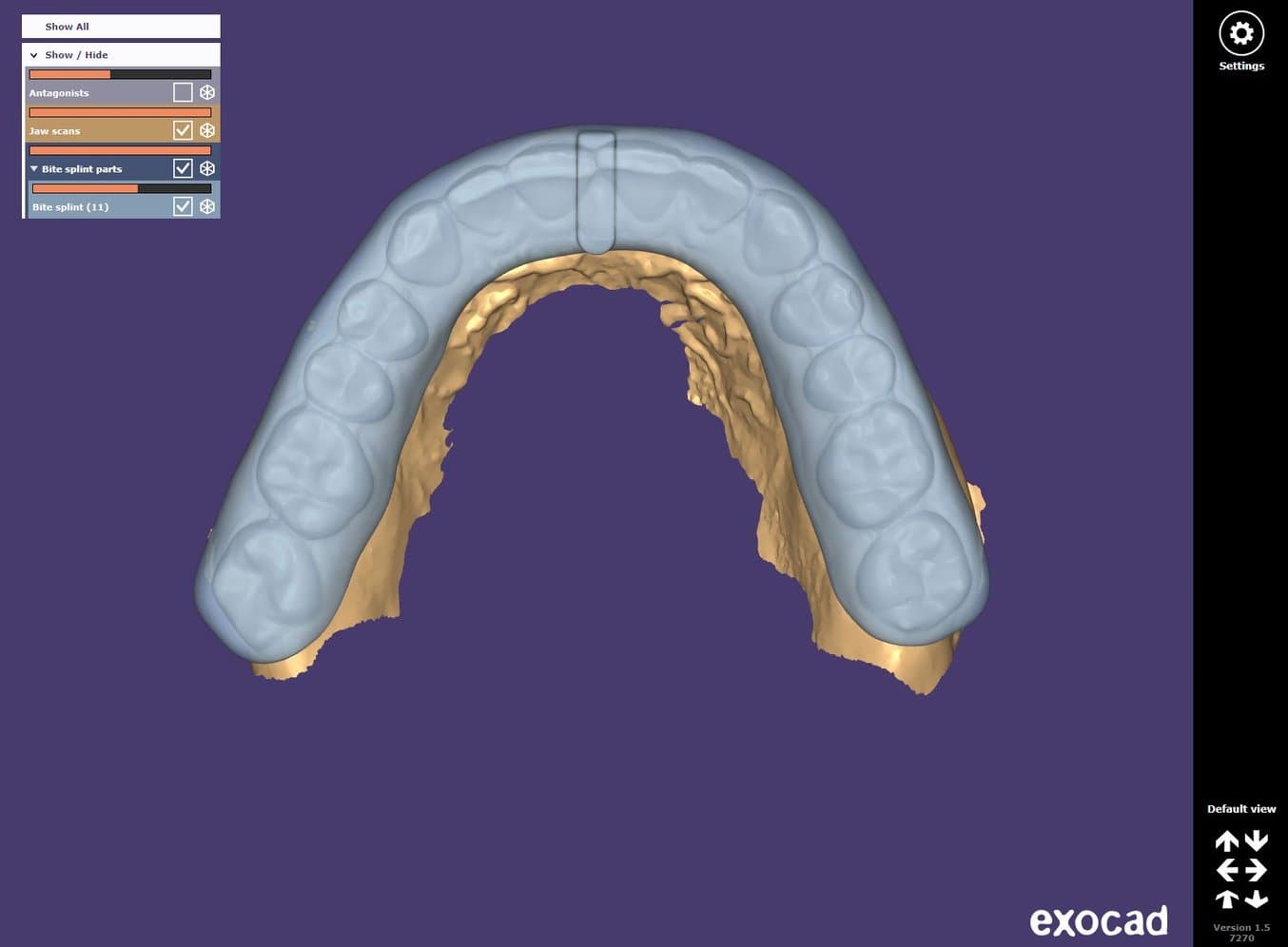
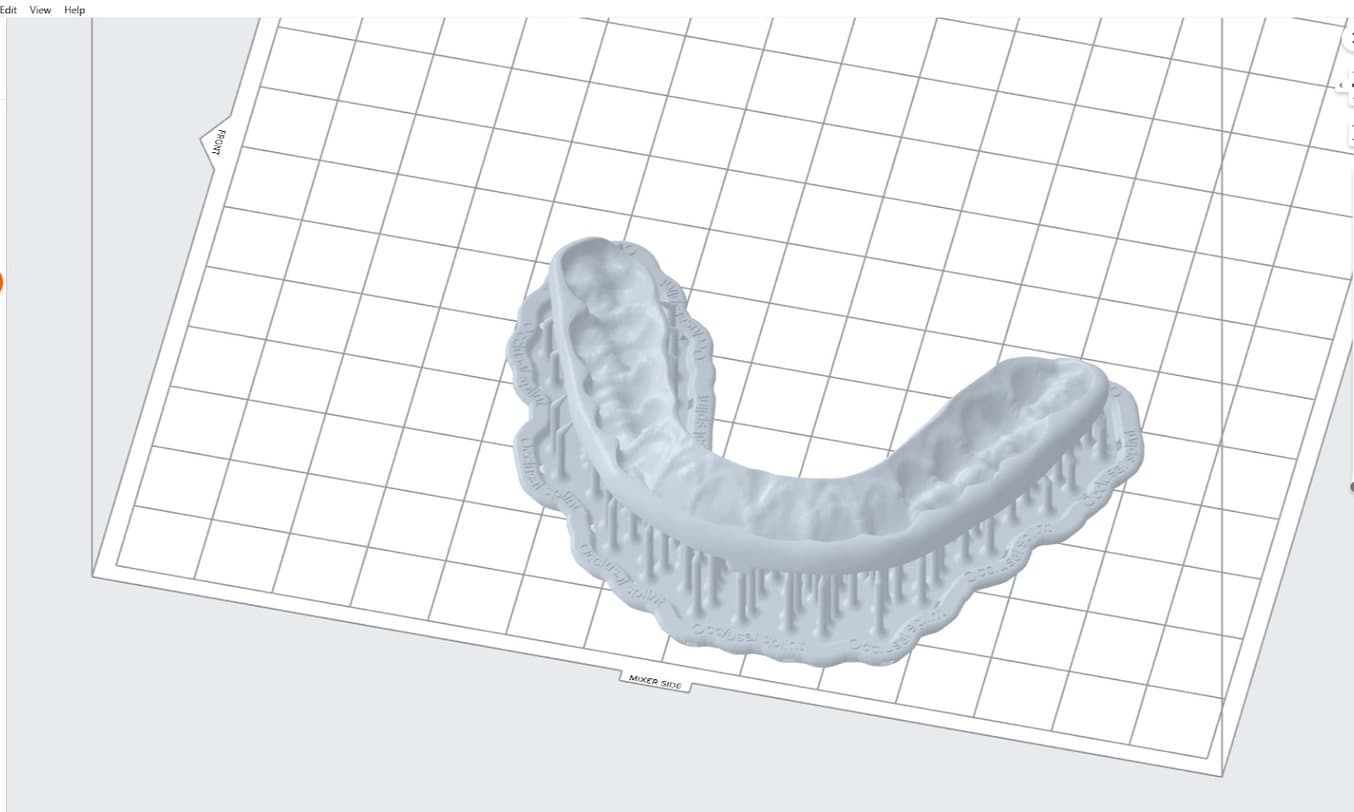
Fig 6. Set-up of the occlusal splint in PreForm as per the Application Guide.
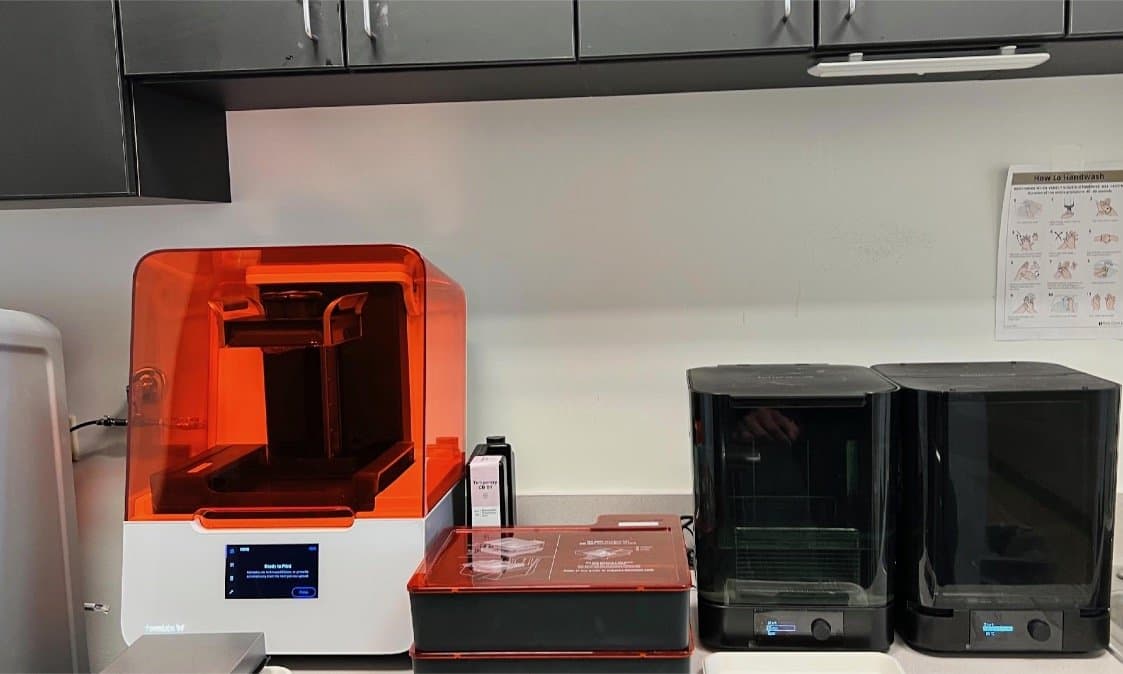
Fig 7. 3D Printing Set-up (Form 3B+, Form Wash and Form Cure)
- Post-processing: The parts were washed for 15 minutes (in a Form Wash containing 99% isopropyl alcohol (IPA)) then removed and washed again in fresh IPA for five more minutes. The parts were dried with compressed air and allowed to air dry completely for 30 minutes. Parts were then cured in the Form Cure at 60°C for 60 minutes. After printing, the build platform was removed from the printer in order to post-process the parts.

Fig 8. Printer occlusal splint and Kois Deprogrammer on a build platform.

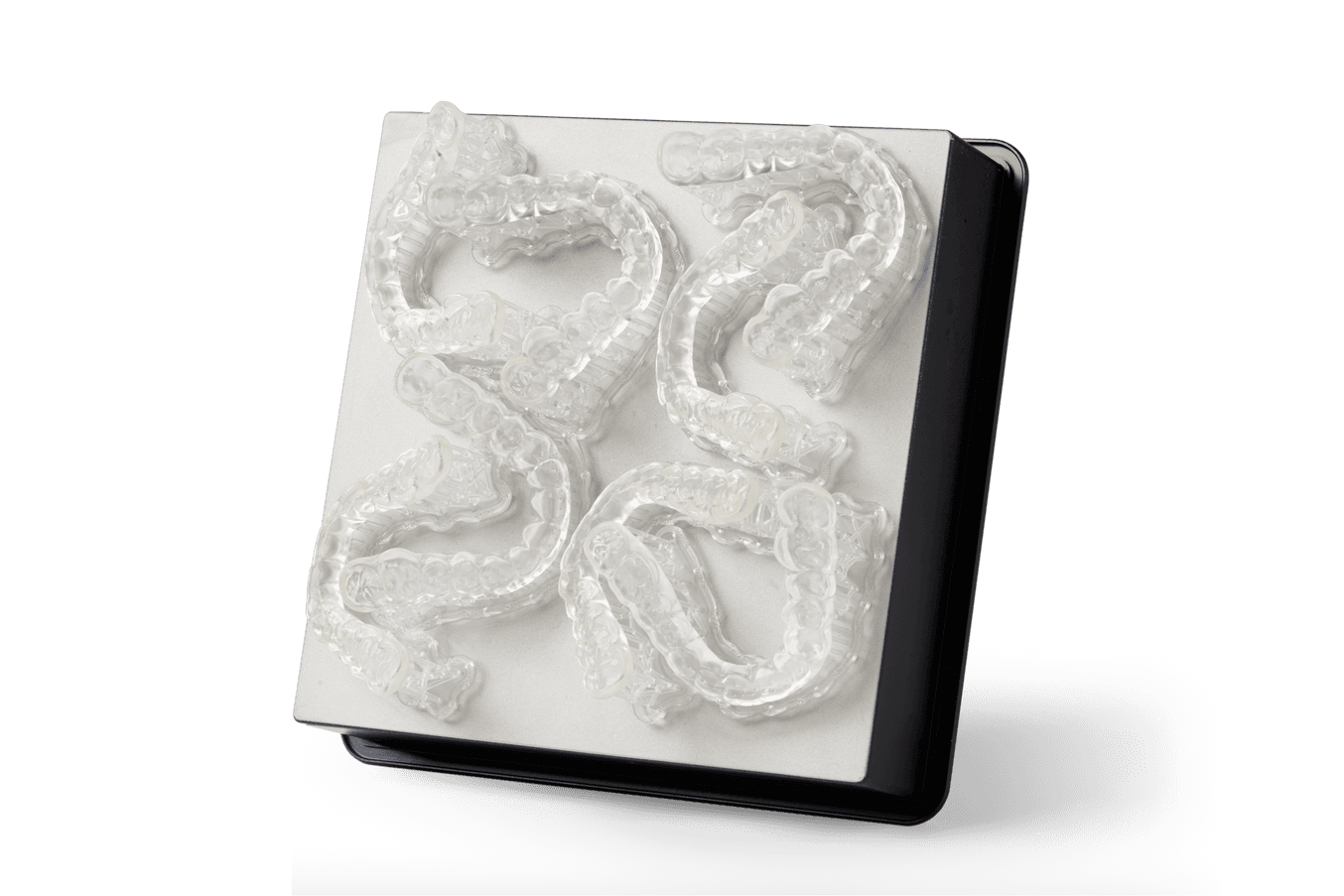
Fig 10. Printed occlusal splint still on support structure, after curing.

Fig 11. Printed occlusal splint still on support structures, after curing, second view.
-
Polishing:
- Support structures were removed and the following polishing steps were taken:
-
A tungsten cross-cut carbide bur was used to remove the support structures indentations in the occlusal surface.
-
A rubber silicone polisher was used to smoothen and even the surface.
-
Finally, a muslin/rag wheel was used for high gloss polishing.

Fig 12-14. Polishing sequence of occlusal splint.


Third appointment (24 hours after the second appointment): The occlusal splint was delivered to the patient. Occlusion was checked and balanced. The patient was instructed on proper cleaning of the appliance with water and a soft brush in addition to reinforcing proper oral hygiene. A follow-up appointment was scheduled for two weeks later for reevaluation of bite on the appliance and compliance for wear of the appliance.

Fig 15. Kois Deprogrammer and occlusal splint after polishing.

Fig 16. Occlusal splint delivered to the patient.
Follow-Ups/Check Ups
Evaluation of splint at the post insertion appointment was completed and the material was holding up well, fit was the same, and the color stability of the material was excellent. The overall patient satisfaction was positive. The patient reported that the fit of the splint was comfortable and easy to insert and remove, and that the material was easy to clean.
Scan to Splint: Automated and Streamlined In-house Splint Production
Join Dr. Christopher Baer to discover how to boost chairside efficiency by integrating your intraoral scanner with in-house 3D printing to create occlusal splints. In this webinar, Dr. Baer will share with you a simple, step-by-step, cost efficient workflow to design and 3D print occlusal splints in-house.
Conclusion
Utilization of a complete digital workflow for fabrication of an occlusal splint in the dental office is a very efficient and cost effective way to provide a high-quality occlusal splint with a short turnaround time. The cost to design and print a splint can be less than $40 with no associated shipping costs; this is significantly lower than a lab fabricated splint. It starts with an intraoral scan that is then electronically sent to an external design service (Evident) for the design team to fabricate the splint. This design process can be done in-house if the office has the proper software, but outsourcing the design can make the process more efficient for the office. Once design is complete, the fabrication begins with 3D printing of the appliance by inserting the correct material and hitting the print button.
Washing and curing of the splint takes a few hours and final polishing can be completed by the dental assistant. Chairside delivery can occur in less than 24 hours after the patient has been scanned and the delivery of the appliance takes only a few minutes. The fit of the appliance can be calibrated by the design team to ensure that the fit is compatible with the practitioner’s preferences. The splint material (Dental LT Clear Resin V2) is clear, and after a quick polishing step looks just like a traditionally fabricated laboratory splint. It should be noted that:
-
Initial fit tests may need to be done to calibrate the clinic scanner, splint design and 3D printer to the clinician’s preferences — similar to the traditional lab process. This can help with the efficiency of the delivery appointment.
-
Digitally designed and printed appliances enable easy replacement should the patient lose or damage the appliance — a new one can be fabricated by simply printing the stored file again. If a patient desires multiple splints, as sometimes is the case when patients travel frequently for work, then the appliance can be printed in duplicated with no additional cost outside of the material.


